
We hear it all the time from our clients— CBCT is a game-changer that allows diagnostic insight that traditional intraoral radiographs simply cannot provide. For certain applications, such as identifying decay, an intraoral radiograph is still one of the best tools in the diagnostic arsenal. For many other applications, such as implant dentistry and endodontics, CBCT is able to easily pick up what could have been missed or misdiagnosed in the 2D image.
Take, for example, this recent case from our client who is a practicing endodontist in the great state of New Jersey:

At first glance, the PA appears to show internal resorption on 10. The CBCT that was acquired on this patient (using the J. Morita X800 F40) shows a different situation:





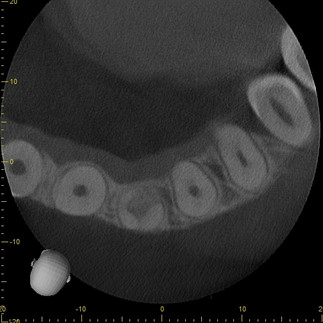
The CBCT scan made clear that this was actually a more rare case of internal resorption that had progressed into replacement resorption. Progressing through the scan, you can actually see that the bone has regrown in such a way that it has completely separated the crown from the apex of the tooth, fundamentally changing the treatment plan for this patient.
The combination of three slice perspectives and the ability to adjust the orientation of the volume allows for a far more comprehensive understanding of pathology or anatomical anomalies.
There is a common saying in medical imaging, "one view is no view," which is made obvious in dentistry on many occasions when comparing a 2D intraoral radiograph to all of the diagnostic information contained in a CBCT volume.